



Vitamin A deficiency is the leading cause of preventable childhood blindness and increases the risk of death from common childhood illnesses such as diarrhea. Periodic, high-dose vitamin A supplementation is a proven, low-cost intervention[1] which has been shown to reduce all-cause mortality by 24 per cent[2], and is therefore critical to achieving Millennium Development Goal 4: to reduce child mortality. The World Health Organization has classified vitamin A deficiency as a public health problem affecting over 250 million children in over half of all countries worldwide, mainly in Africa and South Asia.
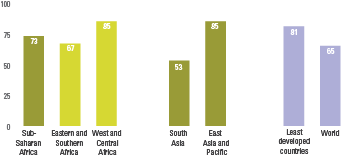
As supplementation is a key child survival intervention, discussions of progress focus largely on coverage of that intervention. Despite the potential benefits, only 65 per cent of targeted children were reached in 2013. The good news is that integrated child health events have helped support high coverage of vitamin A supplementation in 2013 in a large number of least developed countries, where the need is often greatest.

Improving Child Nutrition: The achievable imperative for global progress
This report builds on earlier findings on the impact of undernutrition by highlighting new developments and demonstrating that efforts to scale up nutrition programmes are working, benefiting children in many countries.
GUIDELINES FOR MONITORING VITAMIN A SUPPLEMENT COVERAGE
Guidelines from the Global Vitamin A Alliance (GAVA) are forthcoming and will provide more information on district- and national-level monitoring and reporting of vitamin A supplementation programmes targeted at 6- to 59-month-old children.
THE INDICATOR
The indicator presented on this page, ‘Proportion of 6- to 59-month-olds receiving two high-dose vitamin A supplements in a (given) calendar year’, is defined below.
|
Indicator name (composite) |
Indicator name (for individual semesters) |
Definition |
|
|---|---|---|---|
|
Numerator |
Denominator |
||
|
Proportion of 6- to 59-month-olds receiving two high-dose vitamin A supplements in a (given) calendar year
(The lower coverage value from each of the two semesters in a (given) calendar year
For example, if semester 1 coverage was 70% and semester 2 coverage was 48%, the two-dose coverage estimate would be 48%) |
a) Proportion of 6- to 59-month-olds receiving a high-dose vitamin A supplement in semester 1 (January to June) |
Number of 6- to 59-month-olds reached with one high-dose vitamin A supplement in semester 1 as per total count from the ‘main distribution mechanism’[1] on ‘administrative report’[2] |
Total number of 6- to 59-month-olds in the country |
|
b) Proportion of 6- to 59-month-olds receiving a high-dose vitamin A supplement in semester 2 (July to December) |
Number of 6- to 59-month- olds reached with one high-dose vitamin A supplement in semester 2 as per total count from the main distribution mechanism on administrative report |
Total number of 6- to 59-month-olds in the country |
|
DATA COLLECTION AND REPORTING
Data on coverage of high-dose vitamin A supplementation in 6- to 59-month-old children, which are compiled in UNICEF’s global database, come from administrative reports filled in by national governments, UNICEF country office staff and other partners. The numerators for country-level coverage estimates are generally derived from the following two in-country sources:
- Tally sheets used during outreach or campaign-style events. These can include Child Health Days, Polio National Immunization Days and Measles Supplementary Immunization Activities and capture the total number of doses delivered to children during an event. Tallies from each distribution/event site are summed up to provide the total number reached at the national level.
- Health information system reports capture the total number of supplements delivered through routine health system contacts – that is, the doses delivered to children when they go to a health centre to receive well-child visit services such as vaccinations. These data are generally rolled up to the central level together with information on vaccines or essential drugs.
SELECTION OF COVERAGE DATA FOR THE VITAMIN A PROGRAMME DATABASE
The following rules were used during the 2013 annual review to select or adjust coverage figures for entry into UNICEF’s database and publication in The State of the World's Children.
- National programmes: The database only reports coverage of countries that have programmes that are, or should be, national in scope. Coverage figures are therefore excluded for country programmes that are geographically targeted. For example, coverage data have been excluded for Peru, where specific supplementation efforts regularly reach upwards of 90 per cent of children in areas of the country with an elevated prevalence of vitamin A deficiency or a high under-five mortality rate.
- Nationally representative data: Only ‘nationally representative’ coverage data are included in the database. Since these data are based on administrative reports, the coverage of reporting is used to gauge whether the data are nationally representative. In addition to reporting on the number of children reached in each semester, countries also report on the number of districts (or lower-level administrative units such as health posts) that submitted a report for each semester. Data must be available from at least 80 per cent of districts (or 80 per cent of lower-level administrative units) to be included in UNICEF databases.
- Timing between doses: The amount of time between the distribution dates must be about 4 to 6 months to be included in the database. This is because the protective effects of high-dose vitamin A supplements last about 4 to 6 months. For example, if country A distributed vitamin A supplements during a Child Health Day in March for semester 1, and again in September for semester 2, both of these points would be accepted since they are six months apart, thereby allowing optimal protection. On the contrary, if country B distributed vitamin A supplements through a Child Health Day in June and reported this for semester 1 with 81 per cent coverage, and a Polio National Immunization Day in August reported as semester 2 with 93 per cent coverage, only one of the two points can be used. Even though each event occurred in a different ‘semester’, the short span of time between the two distributions (one to two months between doses) would not confer optimal protection to the children reached. In such a case, the higher of the two (Polio National Immunization Day) would be used and the other point discarded. In the case of country B, the administrative data from routine health system contacts from January to June, if not already submitted through the report, would be sought and, if available, used to report coverage for semester 1. If country B did not have data related to vitamin A supplementation through routine health system contacts for semester 1, the country would be reported as not having data (-) for two-dose coverage for that year in UNICEF’s database.
- Selection of data: Where coverage data from more than one distribution mechanism are available for a given semester, only data from one of them can be used, to prevent double counting of children who may have received a dose through each of the two. When data for both an outreach/campaign style event and routine health system contact are available for the same country in one semester, the coverage estimate is based on only one – the higher of the two. However, since the main distribution mechanisms may vary between sub-age groups of 6- to 11-month-olds and 12- to 59-month-olds, countries are asked to report on these two age groups separately. When numerators and denominators are available for these two main sub-age groups for two different distribution mechanisms in a given semester, they may be combined in different ways, with the aim of giving an estimate with the highest coverage. To take one example: In semester 1, country C reached 90 per cent of 6- to 11-month-olds through routine contact, but only 38 per cent of them through a campaign-style event. It reached 12 per cent of 12- to 59-month-olds through routine contact and 96 per cent of them through an outreach/campaign-style event. In this case, the routine data for 6- to 11-month-olds would be combined with the event data for 12- to 59-month-olds to feed into the overall coverage for 6- to 59-month-olds.
- Adjustment of denominators: When reviewing the denominator data provided through country reports, one of the checks is a comparison with United Nations Population Division estimates for the target age group. Where the denominator in the country report is ≥90 per cent of the UN population estimate, the country-reported denominator is used in conjunction with the country-reported numerator to estimate the coverage. If the country-reported denominator is <90 per cent of the UN estimate, the UN population estimate is used as the denominator in coverage calculations.
- Timely submission of reporting forms: Final reports submitted and cleared prior to 15 September 2014 were included in the The State of the World’s Children 2014. For countries that could not meet this deadline, opportunities to update UNICEF’s global databases are possible at any time pending submission of final reports and clearance of these rules.
- Capped coverage figures: Coverage data points ≥100 per cent were capped at 99 per cent.
- Age-targeted programmes: Coverage for programmes targeting children other than those aged 6 to 59 months are reported as targeted (that is, the proportion of the targeted age range receiving supplements) and marked with a footnote in The State of the World's Children (for example, Viet Nam targets children aged 6 to 36 months in some provinces and 6 to 59 months in other provinces).
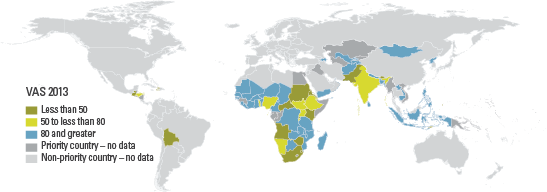
COVERAGE GAPS IN THE DATABASE
Ideally, coverage data are available from all 82 priority countries, that is countries deemed ‘priorities’ for national-level vitamin A supplementation programmes. This would allow aggregated estimates to be representative of the full population of children at risk. However, about one quarter of the 82 priority countries were excluded from the database in 2012 due to non-reporting or data quality concerns. Of all 82 priority countries, 62 had data and were included in the 2012 database. As the countdown advances towards international development goals, further efforts will be needed to ensure timely, accurate and complete reporting on coverage of this critical child survival intervention.
ESTIMATING COVERAGE WITH TWO ANNUAL DOSES
Although international recommendations call for vitamin A supplementation every four to six months, current monitoring efforts are unable to capture the proportion of children covered who are receiving both annual doses of vitamin A. Approximations of two-dose coverage presented here assume that in countries providing more than one round of supplementation, the same children are probably bypassed in both distributions. The proportion of children reached by one campaign but not by the other would be minimal. Therefore, the lower of two coverage data points for a given year is assumed to be roughly equivalent to the proportion of children receiving two doses of vitamin A. UNICEF and its partners are working to develop more refined methods for measuring the proportion of children fully protected.
[1] Main distribution mechanism: Only the main distribution mechanism is used to generate the numerator for a given semester since, in many countries, vitamin A supplementation is often distributed through more than one mechanism, and to avoid double counting, only the mechanism reaching the highest number of children is used in any given semester.
[2] Administrative report: This refers to a variety of potential sources linked to different main distribution mechanisms. For example, if the main distribution mechanism for a given semester is a child health event, a tally sheet is the most common administrative report from which the data would come. If routine distribution through fixed site health posts is the main distribution mechanism, the Health Monitoring information System is the most common administrative report from which data would come. Other common main distribution mechanisms, such as Polio National Immunization Day campaigns and measles campaigns would also generally use tally sheets as their administrative reporting source.