


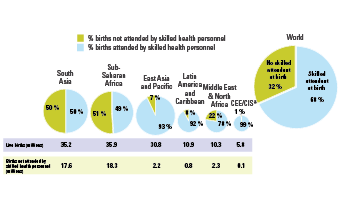

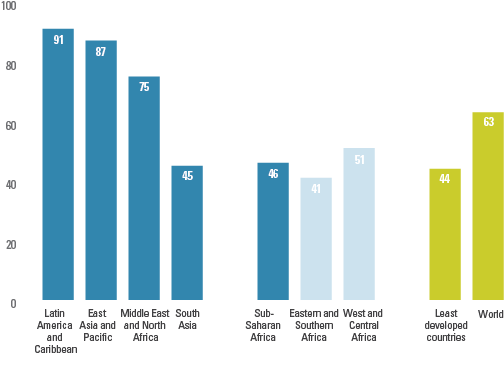
Skilled care during childbirth and access to emergency obstetric care, when required, are the two most critical interventions needed to ensure safe motherhood. Worldwide, about one third of births take place without the assistance of skilled health personnel. In 2014 alone, this translated into more than 40 million unattended births in low and middle income countries, about 90 per cent of which were in South Asia and sub-Saharan Africa.
Sub-Saharan Africa and South Asia, which together represent over 85 per cent of all maternal deaths worldwide, also have the lowest levels of skilled attendance at birth. Regional averages range from about 50 per cent in South Asia and sub-Saharan Africa to a high of 99 per cent in Central and Eastern Europe and the Commonwealth of Independent States (CEE/CIS).
_258.png)

Trends in Maternal Mortality: 1990 to 2013
This report presents new estimates of maternal mortality produced by the Maternal Mortality Estimation Inter-Agency Group (MMEIG) as part of global and country monitoring of the Millennium Development Goal five. The estimates are the seventh in a series of analyses carried out by MMEIG. The report describes estimates of levels and trends in maternal mortality ratio between 1990 and 2013, associated number of maternal deaths and lifetime risk of maternal deaths.
Committing to Child Survival: A Promise Renewed - Progress Report 2014
This report looks at causes of death and coverage of key interventions for mother and newborn and highlights initiatives by governments, civil society and the private sector to accelerate progress on child survival.
UNICEF – in collaboration with WHO – is the UN organization responsible for monitoring and reporting the indicator ‘Births attended by skilled health personnel’, which is one of the official indicators for MDG 5: Improve maternal health.
|
MDG indicator |
Millennium Development Goal |
Target
|
|
5.2 Births attended by skilled health personnel, percentage
|
Goal 5. Improve maternal health |
Target 5.A: Reduce by three quarters, between 1990 and 2015, the maternal mortality ratio |
DEFINITION OF INDICATOR
Births attended by skilled health personnel (doctor, nurse or midwife) is the percentage of births attended by health personnel trained in providing life-saving obstetric care, including giving the necessary supervision, care and advice to women during pregnancy, labour and the postpartum period; conducting deliveries on their own; and caring for newborns. Traditional birth attendants, even if they receive a short training course, are not included.
Computation: The number of live births to women aged 15 to 49 in a defined recent period attended by skilled health personnel (doctor, nurse or midwife), expressed as a percentage of live births to women aged 15 to 49 in the same period.
Measurement limitations: The indicator is a measure of a health system’s ability to provide adequate care for pregnant women. Concerns have been expressed that the presence of a skilled attendant may not adequately capture women’s access to good-quality care, particularly when complications arise, and that information on the supplies and equipment a skilled attendant may or may not have is lacking.
In addition, standardization of the definition of skilled health personnel is sometimes difficult because of differences in training of health personnel in different countries. Although efforts have been made to standardize the definitions of doctors, nurses, midwives (and in some cases, auxiliary midwives) used in most household surveys, it is likely that the abilities of many skilled attendants to provide appropriate care in an emergency depends on the environment in which they work.