


Immunization is one of the most cost-effective public health interventions to date, saving millions of lives1 and protecting countless children from illness and disability. As a direct result of immunization, polio is on the verge of eradication. Deaths from measles, a major child killer, declined by 71 per cent worldwide and by 80 per cent in sub-Saharan Africa between 2000 and 2011.2 And 35 of 59 priority countries have eliminated maternal and neonatal tetanus.
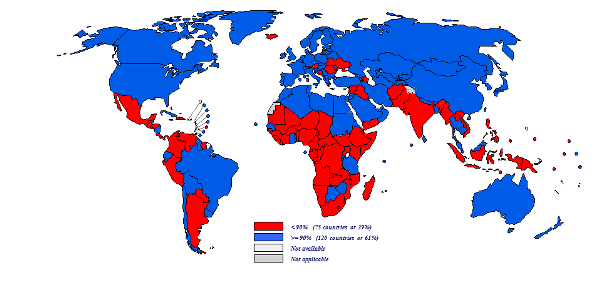
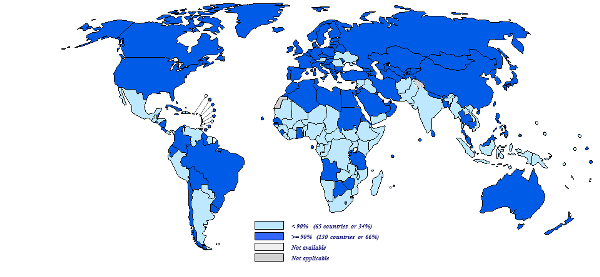
Immunization has not yet realized its full potential, however. As of end-2013, 21.8 million children under 1 year of age worldwide had not received the three recommended doses of vaccine against diphtheria, tetanus and pertussis containing vaccine (DTP3), and 21.6 million children in the same age group had failed to receive a single dose of measles-containing vaccine. Given an estimated annual cohort of 133.6 million surviving infants, an additional 11.2 million children would need to have been reached during 2013 to attain 90% DTP3 coverage globally.
_59.png)

Immunization Summary: A statistical reference containing data through 2013
This immunization summary is a statistical reference containing data through 2013. It was jointly produced by the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO). It presents detailed statistics on the performance of national and district-level immunization systems in 195 countries and territories.

Immunization Coverage Summary Application
The Immunization Summary is an app for visualizing (tables, graphs, maps) data on policies, activities and impact of national immunization systems.
These data are reported by WHO & UNICEF member states annually for incidence, coverage and immunization indicators;
The WHO UNICEF estimates of national immunization coverage constitute an independent technical assessment of coverage;
The population data are provided by the United Nations’ “Population Division. The World Population Prospects - the 2012 revision. New York, 2013.” With the exception of the infant and child mortality figures which are provided by WHO’s “World Health Statistics 2013, data for 2012.”
The GNI & GDP data are taken from "The 2013 World Bank Development Indicators Online".
Data are available from 1980 to 2013 (as of 14 July 2014) for a 195 countries or territories.

Global Routine Vaccination Coverage, 2013
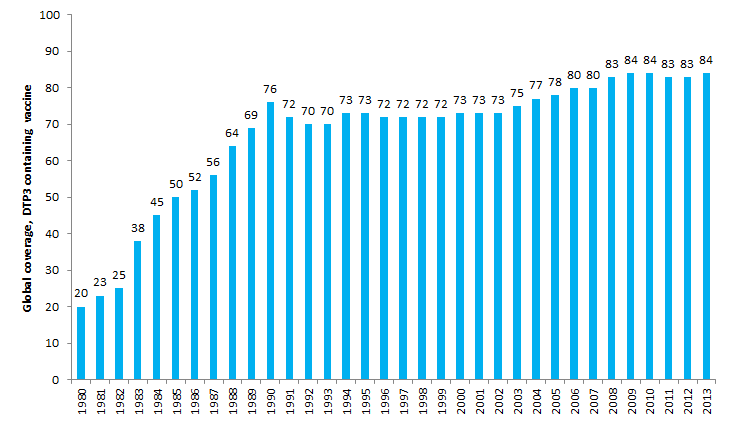
In 1974, the World Health Organization (WHO) established the Expanded Program on Immunization to ensure that all children have access to routinely recommended vaccines. Since then, global coverage with the four core vaccines (Bacille Calmette-Guérin vaccine [for protection against tuberculosis], diphtheria-tetanus-pertussis vaccine [DTP], polio vaccine, and measles vaccine) has increased from <5% to ≥84%, and additional vaccines have been added to the recommended schedule. Coverage with the third dose of DTP vaccine (DTP3) by age 12 months is a key indicator of immunization program performance. Estimated global DTP3 coverage has remained at 83%-84% since 2009, with estimated 2013 coverage at 84%. Global coverage estimates for the second routine dose of measles-containing vaccine (MCV2) are reported for the first time in 2013; globalcoverage was 35% by the end of the second year of life and 53% when including older age groups. Improvements in equity of access and use ofimmunization services will help ensure that all children are protected from vaccine-preventable diseases.
Harris JB, Gacic-Dobo M, Eggers R, Brown DW, Sodha SV. Global Routine Vaccination Coverage, 2013. MMWR Morb Mortal Wkly Rep. 2014;63(46):1055-1058.

Results from a survey of national immunization programmes on home-based vaccination record practices in 2013
During January 2014, WHO and the United Nations Children's Fund sent a one-page questionnaire to 195 countries to obtain information on HBRs including type of record used, number of records printed, whether records were provided free-of-charge or required by schools, whether there was a stock-out and the duration of any stock-outs that occurred, as well as the total expenditure for printing HBRs during 2013.

Home-based record prevalence among children aged 12-23 months from 180 demographic and health surveys
There is currently a re-focus at the global level on the importance of the home-based record within vaccination service delivery as an important information resource but there are few reports of ever and current home-based record prevalence across countries. We considered all Demographic and Health Surveys (starting with DHS round 3) conducted between 1993 and 2013 for which a final dataset was available in the public domain at the time of the analysis.
An electronic copy of the manuscript is available upon request. Please contact us with your requests here
Country-specific reports of the WHO and UNICEF estimates of national immunization coverage
The graphs and data tables displayed in the country-specific reports show the national coverage levels for each vaccine for the period from 2002 through 2013 (see guide
To access country data please click on country name
Central and Eastern Europe and the Commonwealth of Independent States
East Asia and the Pacific
Eastern and Southern Africa
Industrialized countries
Latin America and the Caribbean
Middle East and North Africa
South Asia
West and Central Africa
Since June 2000, WHO and UNICEF have conducted annual reviews of national immunization coverage. Immunization coverage estimates are used for a variety of purposes: to monitor the performance of immunization services at local, national and international levels; to guide polio eradication, measles control and maternal and neonatal tetanus elimination; to identify areas of weak system performance that may require extra resources and focused attention; and as one indicator when deciding whether to introduce a new vaccine. Coverage levels with diphtheria-tetanus-pertussis-containing vaccine (DTP) are considered one indicator of health system performance.
A detailed explanation of the methods behind the WHO and UNICEF estimates of national immunization coverage is provided elsewhere.1,2,3,4 Estimates of immunization coverage are generally based on two sources of empirical data: reports of vaccinations performed by service providers (administrative data5) and household surveys containing items on children's vaccination history (coverage surveys). For estimates based on administrative data, the immunization coverage is derived by dividing the total number of vaccinations given by the number of children in the target population. For most vaccines the target population is the national annual number of births or number of surviving infants (this may vary depending on countries' policies and the specific vaccine). Immunization coverage surveys are frequently used in connection with administrative data. The Expanded Programme on Immunization (EPI) 30-cluster survey, the UNICEF-supported Multiple Indicator Cluster Surveys (MICS) and the Demographic Health Surveys (DHS) supported by the United States Agency for International Development are the principal surveys used as sources of information on immunization coverage.
This review relies on the following data:
- Officially reported data by WHO and UNICEF Member States
- A historical database maintained by UNICEF
- Nationally representative, population-based household survey reports (published and unpublished).
It is important to distinguish whether data accurately reflect immunization system performance or whether they are compromised and thus present a misleading view of immunization coverage. Officially reported data are therefore compared with independent surveys. Based on the data available, the consideration of potential biases and the contributions of local experts, the most likely level of immunization coverage is determined for each country–year–antigen combination. An essential part of this review is consultation and collaboration with national authorities, who are asked to review the draft estimates and provide comments.
- Burton, A., et al., ’A Formal Representation of the WHO and UNICEF Estimates of National Immunization Coverage: A computational logic approach’, PLOS ONE, vol. 7, no. 10:e47806, 2012.
- Kowalski R., A. Burton, ’WUENIC – A Case Study in Rule-based Knowledge Representation and Reasoning’, Lecture Notes in Computer Science, vol. 7258, 2012, pp. 112─125.
- Burton, A., et al., WHO and UNICEF Estimates of National Infant Immunization Coverage: Methods and processes, Bulletin of the World Health Organization, vol. 87, 2009, pp. 535─541.
- Brown DW, Burton AH, Gacic-Dobo M, Karimov RI. An Introduction to the Grade of Confidence Used to Characterize Uncertainty Around the WHO and UNICEF Estimates of National Immunization Coverage. Open Public Hlth J. 2013;6:73-76.
- Administrative data are collected through the WHO/UNICEF Joint Reporting Form on Vaccine-Preventable Diseases, completed annually by countries.
ImmunizationInfo: Expanding access to national immunization coverage estimates
The data above can also be viewed through ImmunizationInfo, an interactive online dissemination tool of national childhood immunization coverage statistics developed in 2010 by UNICEF and WHO in collaboration with Community Systems Foundation. ImmunizationInfo is powered by DevInfo database technology and built using Adobe-Flex technology and allows users to view national immunization coverage estimates in graph, map and table formats based on a user-defined selection of country-year-vaccine combinations. Users can generate comparative graphs and also download the underlying data.