


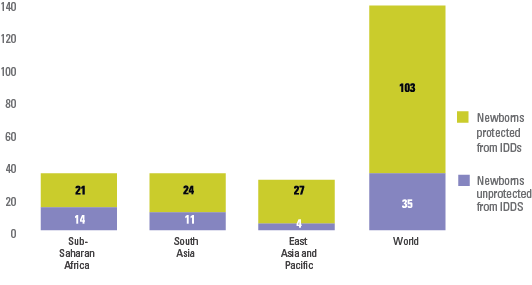
Iodine deficiency can lead to a variety of health and developmental consequences known as iodine deficiency disorders (IDDs). Iodine deficiency is especially damaging during the early stages of pregnancy and in early childhood. In their most severe forms, IDDs can lead to cretinism, stillbirth and miscarriage; even mild deficiency can cause a significant loss of learning ability. In 2013, more than 35 million newborns were unprotected from the lifelong consequences of brain damage associated with iodine deficiency.
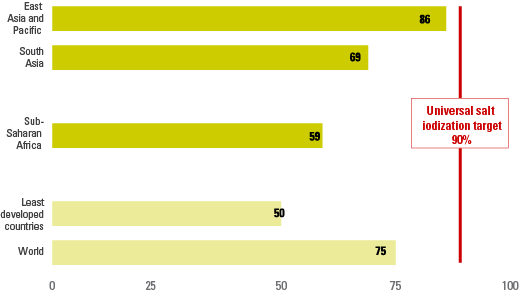
For the last 30 years, universal salt iodization has been the most widely used strategy to control and eliminate IDDs. The target aims for consumption of adequately iodized salt in more than 90 per cent of households. However, this goal is a long way from being met.

MONITORING ELIMINATION OF IODINE DEFICIENCY DISORDERS
A set of guidelines for monitoring IDD control programmes with both process and impact indicators are described in the World Health Organization (WHO) manual, Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination. With regard to process, it is important to monitor salt iodine content at the levels of production/importation, retail/wholesale sales, and in the household (consideration should also be given to assessing the use of iodized salt in the food industry, where relevant). To monitor impact, median urinary iodine is the main indicator for assessing a population’s iodine status, with total goitre prevalence providing additional useful information. WHO maintains a database on programme impact with indicators related to urinary iodine and goitre prevalence.[1] UNICEF maintains a database on household consumption of iodized salt. Currently, no agency is responsible for reporting on other process-related indicators regarding production, importation or sales. Ideally, the entire set of process indicators should be combined with impact data to best guide programmes and policies in individual countries.
THE INDICATOR
The indicator presented on this page, ‘Proportion of households consuming adequately iodized salt’, provides part of the picture with regard to monitoring IDD elimination efforts.
|
Indicator name |
Definition |
|
|---|---|---|
|
Numerator |
Denominator |
|
|
Proportion of households consuming adequately iodized salt |
Number of households with salt iodine content ≥ 15 parts per million (ppm) |
Number of households surveyed with salt tested for iodine content and households without salt |
The indicator definition for adequately iodized salt specifies a minimum of 15 parts per million (ppm) of iodine in salt. The amount of iodine in salt samples is important to assess: To be fully effective in correcting iodine deficiency, salt with iodine must not only reach the entire affected population, it also needs to have enough (yet not too much) iodine. While some countries may have different targets, the WHO recommendation is to have 15 to 40 ppm of iodine for salt at the household level, thus the definition used is ≥ 15 ppm.
The assessment of iodine content has generally been accomplished through the use of rapid test kits. While the test kit cannot provide data that are as precise and accurate as titration, it remains the test method associated with most data points in UNICEF’s global database. Based on recommendations from WHO to only use rapid test kits to indicate the presence of iodine, and to use another method – titration – to quantify and report on salt with a particular amount of iodine, a number of countries have stopped reporting on the cut-off of ≥15 ppm and only report on salt with any iodine (>0 ppm) in many recent surveys.
DATA COLLECTION AND REPORTING
Data for household consumption of adequately iodized salt are collected mainly though nationally representative household surveys, such as MICS and DHS. A more limited number of national estimates in the UNICEF global database come from primary school-based surveys or surveillance systems in countries where the primary school net enrolment rate exceeds 90 per cent.
LIMITATIONS
There are a variety of limitations associated with reporting on progress in household consumption of adequately iodized salt, many of them linked to advancements in methodologies and programme maturation. Great strides have been made in enhancing programme monitoring, leading to increased availability and improved quality of data over the past decade. At the same time, they render older data points non-comparable to newer ones, thereby limiting the ability to undertake trend analyses. Some key issues are highlighted below:
Shift from monitoring production to household consumption
- Questions about household consumption of iodized salt were only added to major household surveys starting in the mid-1990s. And even then, not all countries had estimates based on household data. In the early to mid-1990s, many national estimates presented in UNICEF’s annual report The State of the World’s Children were based on extrapolations from iodized salt production figures. Since these estimates are not comparable to the current household consumption-based data, they cannot be used for trend analysis.
Testing for iodine in household salt samples
- Self-reporting: Although the move from production to household consumption-based estimates was a positive one, it still introduced some bias since early estimates were often based on self-reporting. Even some early DHS did not test household salt for the presence of iodine, relying on self-reporting by the respondent or a cross-check against the label/brand name of the salt by the survey interviewer. These self-reported estimates are not comparable to the current household consumption-based data, and cannot therefore be used for trend analyses.
- Rapid test kits: These kits allow for semi-quantification of iodine content and were introduced into many surveys in the mid- to late 1990s as a means of cross-checking a sample of salt within the household during the survey. This helped in decreasing the bias of estimates based on self-reporting from household survey data and represents one of the first examples of direct testing in household surveys. Currently, nearly all MICS and DHS as well as most other national household surveys/monitoring mechanisms include a salt-testing component using rapid test kits for iodine.
- Titration: The most recent WHO recommendation is to use titration to quantify iodine content in salt samples gathered through household surveys. These recommendations also call for use of rapid test kits to indicate presence of iodine only, not adequate iodine (>15 ppm). Since the use of titration has been slow to catch on, and with many countries only reporting on salt with any iodine based on rapid test kits, the ability to construct trends has been further compromised.
- The maximum threshold for iodine in salt is not considered: In attempting to measure ‘adequate’ iodine in salt, the most frequent test method (rapid test kits) look only at the minimum – and not maximum – amount. However, excess iodine can also lead to health problems, and the absence of an acceptable upper range in most data points available limits the interpretability of the data.
- Country-specific iodine targets: Some countries have alternate targets for iodine in salt (for example, neither ≥ 15 ppm nor 15–40 ppm) based on their specific salt consumption patterns, the availability of iodine through sources other than table salt, etc. This further complicates the ability to compare data over time and across countries.