


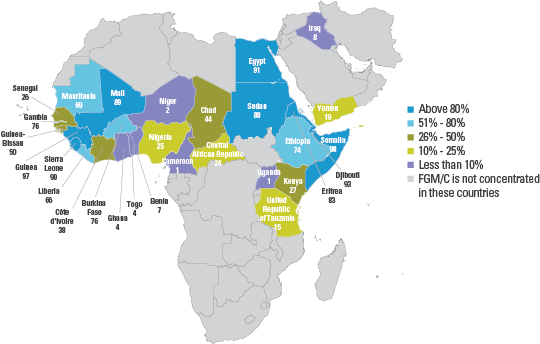
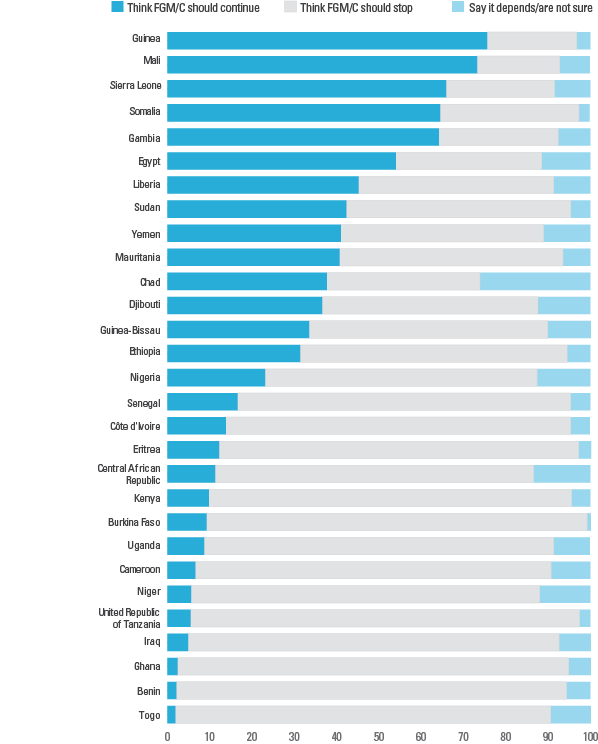
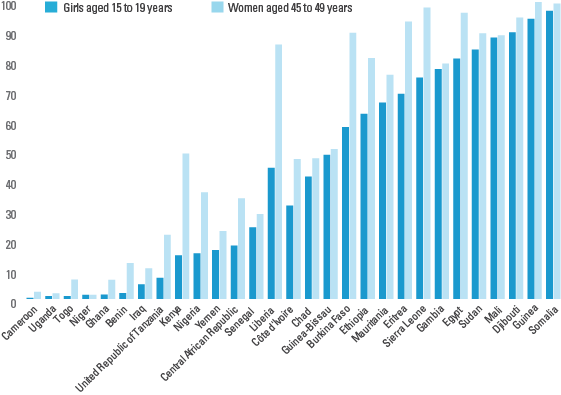
Female genital mutilation/cutting (FGM/C) refers to “all procedures involving partial or total removal of the female external genitalia or other injury to the female genital organs for non-medical reasons.”[1] FGM/C is a violation of girls’ and women’s human rights. Yet where it is still practised, FGM/C is performed in line with tradition and social norms and is strongly associated with ethnicity. More than 130 million girls and women alive today have been cut in the 29 countries in Africa and the Middle East where FGM/C is concentrated. If current trends continue, as many as 30 million girls are at risk of being cut before their 15th birthday. However, the data also show that the majority of girls and women in most practising countries think FGM/C should end. The practice is less prevalent among adolescent girls than among their middle-aged counterparts in most of the 29 countries.

Female Genital Mutilation/Cutting: A statistical overview and exploration of the dynamics of change
This report is a comprehensive statistical overview of female genital mutilation/cutting (FGM/C) in the 29 countries where the practice is concentrated. Analysis of the data reflects current perspectives on FGM/C, informed by the latest policy, programmatic and theoretical evidence.

Female Genital Mutilation/Cutting: A statistical overview and exploration of the dynamics of change, Executive Summary
This report is a comprehensive statistical overview of female genital mutilation/cutting (FGM/C) in the 29 countries where the practice is concentrated. Analysis of the data reflects current perspectives on FGM/C, informed by the latest policy, programmatic and theoretical evidence.




Female Genital Mutilation/ Cutting Country Profiles
These statistical profiles present the latest available data on female genital mutilation/cutting (FGM/C) for 30 countries where FMG/C is concentrated. They provide figures on how widespread the practice of FGM/C is, when and how it is performed, and what women and men think about the practice. Trends in prevalence and attitudes are also presented.
DATA SOURCES
Nationally representative data on FGM/C are mainly available from two sources: Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS). In some countries, data have been collected through other nationally representative household surveys.
A module on FGM/C was developed for the first time for the 1989–1990 DHS conducted in the northern part of what was then known as Sudan. After a few years, the module was modified and has been included in DHS for 23 countries to date. The first module on FGM/C was included in the 2000 MICS in the Central African Republic, Chad and Sudan. The third and fourth rounds of MICS (mainly conducted in 2005–2006 and in 2009─2011) generated updated FGM/C data from 16 countries, including 7 with no prior data (Djibouti, the Gambia, Guinea-Bissau, Iraq, Sierra Leone, Somalia and Togo). Over the last 10 years, UNICEF and ICF International have worked closely to standardize survey questions on FGM/C used in DHS and MICS.
MAIN INDICATORS
The first indicator for measuring FGM/C prevalence is the percentage of girls and women of reproductive age (15 to 49) who have experienced any form of the practice. This is derived from self-reports. Typically, girls and women are also asked about the type of FGM/C performed, at what age they were cut and by whom. Most surveys include additional questions related to women’s – and in some cases men’s – attitudes surrounding FGM/C. In most surveys, eligible respondents are all girls and women aged 15 to 49. Exceptions include Egypt (DHS in 1995, 2000, 2003 and 2005), Sudan (DHS 1989─1990) and Yemen (DHS 1997), where the sample of respondents includes only girls and women aged 15 to 49 who have ever been married.
The second indicator used to report on the practice measures the extent of cutting among daughters of girls and women of reproductive age (15 to 49). In surveys up to 1999, female respondents who had at least one living daughter were asked about their eldest daughter: whether she was cut, the age at which FGM/C was performed, the type of FGM/C carried out and the person who did it. If the eldest daughter was reportedly not cut, respondents were asked if they intended to have their daughter cut. Starting in 1999, rather than asking about the eldest daughter, DHS and MICS began asking respondents whether any of their daughters had undergone FGM/C and, if so, how many of their daughters had been cut. This was followed by questions about the procedure (type, age at cutting and practitioner) for the daughter most recently cut.
Survey data on the FGM/C status of only one daughter cannot be used to estimate the prevalence of FGM/C among girls under age 15. To address this limitation, MICS and DHS in 2010 introduced changes in the standard methodology used to collect information on FGM/C among daughters. The new module asks all girls and women aged 15 to 49 about the FGM/C status of all of their daughters under age 15. As a result, prevalence estimates can be obtained for girls aged 0 to 14. A key point to be kept in mind is that the prevalence data for girls aged 0 to 14 reflect their current, but not final, FGM/C status, since some girls who have not been cut may still be at risk of experiencing the practice once they reach the customary age. Therefore, the data on prevalence for girls under age 15 is actually an underestimation of the true extent of the practice. Since age at cutting varies among settings, the amount of underestimation also varies. This should be kept in mind when interpreting all FGM/C prevalence data for this age group. Prevalence data on girls aged 0 to 14 can be used to assess the impact of recent efforts to end FGM/C since this is the age group most recently cut or at imminent risk of being cut.
INTERPRETING THE DATA
Data on FGM/C inform policymakers of critically important variables in an effort to better understand the practice and develop policies for its abandonment. That said, these data must be analysed in light of the extremely delicate and often sensitive nature of the topic.
Self-reported data on FGM/C need to be treated with caution for several reasons. First, women may be unwilling to disclose having undergone the procedure because of the sensitivity of the topic or the illegal status of the practice in their country. In addition, women may be unaware that they have been cut or of the extent of the cutting, particularly if FGM/C was performed at an early age.
Information on the FGM/C status of daughters is generally regarded as more reliable than women’s self-reports, since any cutting would have occurred relatively recently and mothers presumably would have had some involvement in or knowledge of the event. However, even these data need to be interpreted with a degree of caution. Mothers may be reluctant to disclose the actual FGM/C status of their daughters for fear of repercussions, especially in countries where the practice has been the target of campaigns or legal measures to prohibit it.
With increased availability of nationally representative data on FGM/C, including repeat surveys in several countries, trends in the prevalence and attitudes towards the practice can be analysed. Despite this, considerable challenges arise when examining trends, particularly when establishing a connection between programmatic activities and changes in prevalence levels over time.
First, prevalence can be compared from surveys in the same country from two (or more) points in time. Second, a trend analysis can examine FGM/C prevalence at one point in time across five-year age cohorts for girls and women aged 15 to 49. Finally, current prevalence among girls and women aged 15 to 19 and ‘adjusted’ prevalence among girls aged 10 to 14 can be analysed. Several important factors should be considered when examining trends in the practice:
- Variations in the number of years between consecutive surveys. This can range from 1 to up to 20, depending on the country.
- The number of data points available for each country. Patterns of change are more evident when several surveys are available, as opposed to two data sources.
- The retrospective periods involved (that is, time lags). For instance, in the case of a country where girls are cut before 1 year of age, most girls in the youngest cohort (15 to 19 years of age) are generally reporting on an event that took place 14 to 18 years previously. Any change that occurred after this period will therefore not be reflected in the data.
- The magnitude of change. Change can be gauged by looking either at the absolute difference (change in percentage points) between estimates or at the percentage change between estimates. Conclusions should be drawn on the basis of both measures.
-
Survey design and implementation. This could include, for example, changes in sampling frames, questionnaire content and structure, and language used to refer to the practice.
More detailed discussion of data collection methodologies and assessment of trends related to FGM/C can be found in: Female Genital Mutilation/Cutting: A statistical overview and exploration of the dynamics of change.
MICS MODULE ON FGM/C
MICS surveys have a standardized module for female genital mutilation/cutting.