


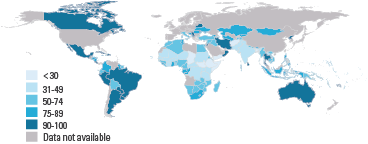

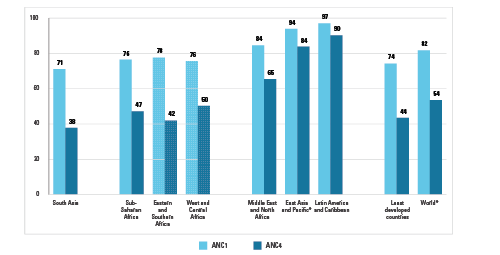
Regular contact with a doctor, nurse or midwife during pregnancy allows women to receive services vital to their health and that of their future children. The World Health Organization (WHO) recommends a minimum of four antenatal care visits. However, global estimates indicate that only about half of all pregnant women receive this recommended amount of care.
Antenatal care can help women prepare for delivery and understand warning signs during pregnancy and childbirth. It can be a source for micronutrient supplementation, treatment of hypertension to prevent eclampsia, immunization against tetanus, HIV testing and medications to prevent mother-to-child transmission of HIV in cases of HIV-positive pregnant women. In areas where malaria is endemic, health personnel can also provide pregnant women with medications and insecticide-treated mosquito nets to help prevent this debilitating, sometimes deadly disease.

Trends in Maternal Mortality: 1990 to 2013
This report presents new estimates of maternal mortality produced by the Maternal Mortality Estimation Inter-Agency Group (MMEIG) as part of global and country monitoring of the Millennium Development Goal five. The estimates are the seventh in a series of analyses carried out by MMEIG. The report describes estimates of levels and trends in maternal mortality ratio between 1990 and 2013, associated number of maternal deaths and lifetime risk of maternal deaths.
UNICEF – in collaboration with the World Health Organization (WHO) – is the UN organization responsible for monitoring and reporting on indicators in antenatal care coverage: at least one visit with a skilled health provider and at least four visits with any provider. Both are official indicators for MDG 5: Improve maternal health.
|
MDG indicator |
Millennium Development Goal |
Target
|
|
5.5 Antenatal care coverage (at least one visit with a skilled provider)
Antenatal care coverage (at least four visits with any provider) |
Goal 5. Improve maternal health |
Target 5.B: Achieve, by 2015, universal access to reproductive health |
DEFINITION OF INDICATORS
Antenatal care coverage (at least one visit) is the percentage of women aged 15 to 49 with a live birth in a given time period that received antenatal care provided by skilled health personnel (doctor, nurse or midwife) at least once during pregnancy.
Skilled health personnel refers to workers/attendants that are accredited health professionals – such as a midwife, doctor or nurse – who have been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth and the immediate postnatal period, and in the identification, management and referral of complications in women and newborns. Both trained and untrained traditional birth attendants are excluded.
Antenatal care coverage (at least four visits) is the percentage of women aged 15 to 49 with a live birth in a given time period that received antenatal care four or more times. Available survey data on this indicator usually do not specify the type of the provider; therefore, in general, receipt of care by any provider is measured.
Antenatal visits present opportunities for reaching pregnant women with interventions that may be vital to their health and well-being and that of their infants. WHO recommends a minimum of four antenatal visits based on a review of the effectiveness of different models of antenatal care. WHO guidelines are specific on the content of antenatal care visits, which should include:
· blood pressure measurement
· urine testing for bacteriuria and proteinuria
· blood testing to detect syphilis and severe anaemia
· weight/height measurement (optional).
Measurement limitations. Receiving antenatal care during pregnancy does not guarantee the receipt of interventions that are effective in improving maternal health. Receiving antenatal care at least four times, which is recommended by WHO, increases the likelihood of receiving effective maternal health interventions during antenatal visits. Importantly, although the indicator for ‘at least one visit’ refers to visits with skilled health providers (doctor, nurse or midwife), ‘four or more visits’ refers to visits with any provider, since standardized global national-level household survey programmes do not collect provider data for each visit. In addition, standardization of the definition of skilled health personnel is sometimes difficult because of differences in training of health personnel in different countries.